
Against the Current, No. 27, July/August 1990
-
A Non-Peace Non-Dividend?
— The Editors -
Black Workers for Justice
— an interview with Nathanette Mayo -
Building from the Grassroots
— Cynthia Bowens -
U.S.C. Out of South Africa
— Harry Brighouse, John Hayes and Michele Milner -
Abortion Pill Is No Panacea
— Joan Batista -
RU 486 Is in the Spotlight
— Joan Batista -
Ford Battles Mexican Workers
— Dianne Feeley -
Soviet Jewish Immigration: Gift or a Time Bomb?
— Michel Warshawski -
The Cancer Epidemic, Part I
— James Morton -
Tracking the Rise of an Epidemic
— James Morton -
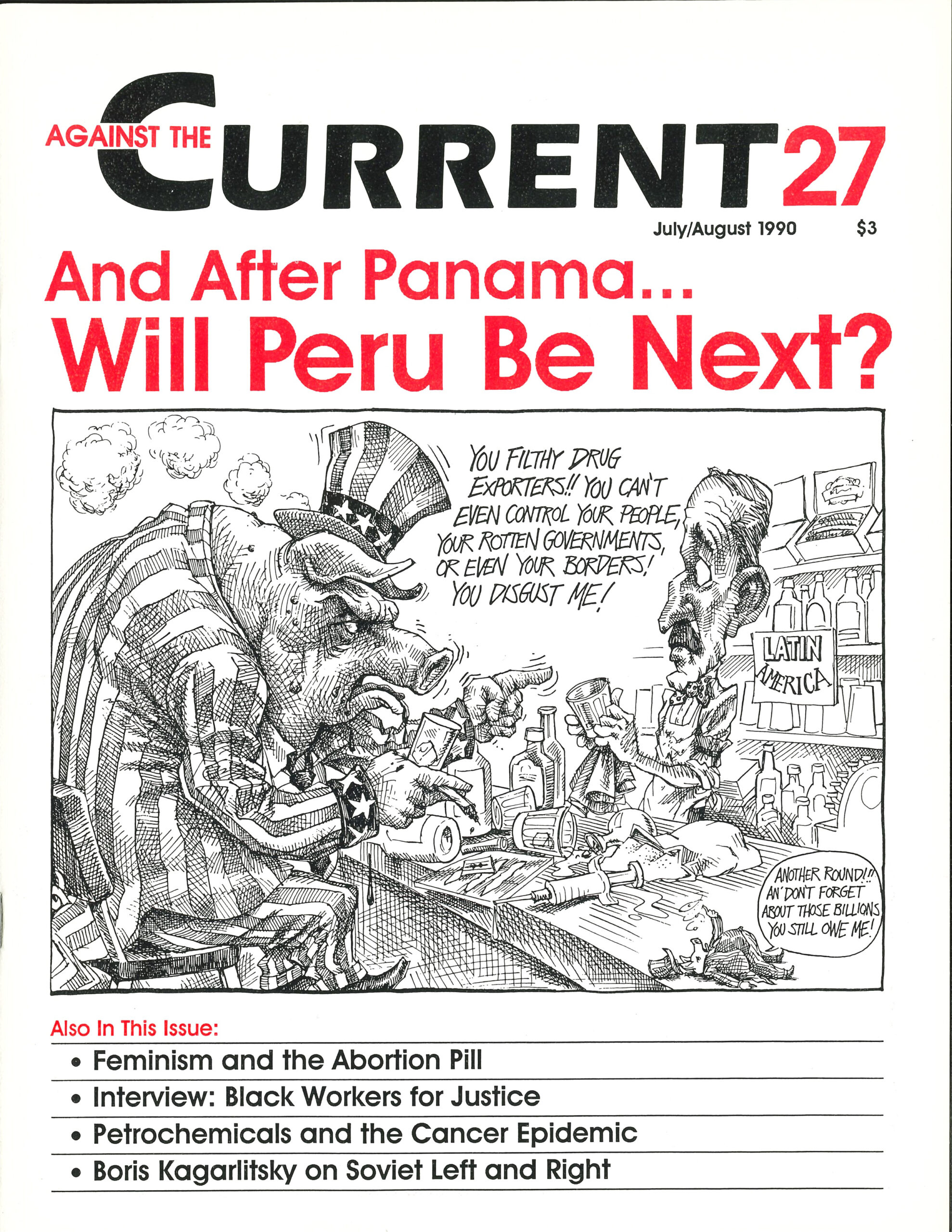
Drug Wars and the Empire
— Peter Drucker -
Mujahideen and Dealers
— Peter Drucker -
The Meaning of the Puerto Rican Plebiscite
— The Taller de Formación Política (TFP) -
Soviet Struggle: What is "Left" and "Right"?
— Boris Kagarlitsky -
Dialogue: The Third World After the Cold War
— James Petras and Mike Fischer -
The Afghans' Tragic Drama
— Val Moghadam -
Afghan: Socialism from Above and Outside
— Samuel Farber -
Random Shots: Summertime Musings
— R.F. Kampfer
Joan Batista
RU 486 HAS BEEN touted as a revolutionary way for women to terminate a pregnancy, a pill that allows a woman to abort in the privacy of her own home. The urgency felt by those of us in the pro-choice movement—especially since the Webster decision—to maintain legal and accessible abortion for all women has led many feminists to uncritically herald RU 486. This seems to flow almost automatically, given the right-wing’s attempt to prevent the drug from being brought into the United States for testing.
For those who champion the right of women to control our own bodies, the battle over RU 486 has so far not been subject to much in-depth discussion. The impression that most people have, and seem to want to keep, both in mainstream women’s groups and on the left—some “radical” women’s groups and feminist health centers excepted—is that RU 486 is a miracle drug that will alter the abortion debate forever.
But feminists must examine RU 486 critically. Especially for women of color, birth control research has often been carried out without the necessary safeguards for women’s health. The way research is funded and carried out, the way scientific journals and the media report on the research—all suggest that reproductive-rights activists must carefully examine the claims for RU 486. Are they exaggerated? What are the real dangers women who take RU 486 face?
The effort to test, produce and distribute this drug in the United States relies heavily on the idea that RU 486 is an effective, safe, cheap and private means to terminate a pregnancy. Unfortunately, this may be wishful thinking.
The hopes pinned on this drug and the growing concentration on efforts to get it into the United States could have dangerous effects on the reproductive rights movement as a whole. Moreover, the drug itself could have dangerous effects on women’s bodies.
What is the Abortion Pill?
RU 486, also known as mifepristone, is an oral steroid hormone that blocks the effects of the hormone progesterone. Progesterone normally causes an increase in the lining of the uterus, allowing for the implantation of the fertilized egg. It also acts to prevent uterine contractions during pregnancy.
With RU 486, the uterine lining breaks down and the fertilized egg is eventually expelled. To increase the likelihood of a complete expulsion, prostaglandin, a chemical that induces contractions, is administered either by injection or vaginal suppository 3648 hours after the ingestion of RU 486.
Because the procedure interrupts the fetal gestation continuum (from the generation of egg and sperm to birth of a baby), its developer calls RU 486 a “contragestive.”(1) The anti-progesterone compound is available for popular use only in France.
By law, four visits to a health-care professional are required to use the drug. The first visit is to verify a pregnancy of seven weeks or less, to check for ectopic pregnancy, and to screen and counsel women interested in using the drug. The drug itself is administered on the second visit in the form of three 200 mg pills.
Thirty-six to forty-eight hours later, the prostaglandin analogue is administered at the clinic and the woman stays there and is monitored for four hours. Most of the women studied have aborted after the supervised four-hour period. A fourth visit is necessary to ensure that the abortion was completed.
There is currently a success rate of 96 percent when these guidelines are followed.(2) The remaining four percent must have a surgical abortion to guard against infection or possible birth defects, as well as to terminate the pregnancy.
Side effects from RU 486 include heavy and prolonged bleeding (lasting from two to thirty-five days), abdominal pain, and cramping. Side effects of the prostaglandin analogue include nausea, vomiting, diarrhea and cramping.
One percent of women using RU 486 have bled heavily enough to warrant a blood transfusion. Studies have also shown that the procedure sometimes suppresses ovulation for three to seven months and has some undetermined effects on the adrenal gland. There are also numerous contraindications.(3)
The most recent test results reported in the New England Journal of Medicine (3/8,90) relate that, for unexplained reasons, the speed of the abortion, the intensity of abdominal pain, and the duration and intensity of the bleeding depend on the type and dosage of prostaglandin analogue administered. Higher dosages speed the expulsion with greater pain and more hemorrhaging.
The procedure has been tested on humans only since 1982. The eight years of testing it has undergone is about half the time normally needed to determine any major, long-term effects of drugs.
Political Baffles over Use
RU 486 was developed by a French scientist, Dr. Etienne-Emile Baulieu, who has been retained as a consultant by the French company Groupe Roussel-Uclaf, a subsidiary of the German pharmaceutical giant Hoechst AG. The French government also owns 36 percent of its stock.
The drug was first tested in Switzerland, and testing has also been conducted in France, Great Britain, the United States and India among others. It was cleared for use in France in September 1988, but distribution was suspended one month later by Roussel-Uclaf. The company cited threats of boycotts and violence by anti-choice extremists as the reason for the withdrawal.
The company’s announcement was greeted with public and professional protest. The French Minister of Health ordered Roussel-Uclaf to resume distribution, calling the drug “the moral property of women,” and threatening to possibly transfer the patent for RU 486 to the government as is allowed by French law. Roussel-Uclaf quickly obeyed.
It has been alleged in the French press that Roussel-Uclaf not only expected the public outcry but also manipulated the decision-making process, in effect, engineering a public consensus that absolved them of the responsibility for the controversial drug while not absolving them from the potentially huge profits.
Since then, RU 486 has been available in clinics in France that are legally authorized to terminate pregnancy. Roussel-Udaf has no immediate plans for distribution of the drug outside of France, although they have cooperated with testing of it in Britain, Sweden, and the Netherlands. The company has also shown interest in cooperating with future testing in California.(4)
Mifepristone is also being used in China and could be synthesized now in South Korea and Hungary. The World Health Organization (WHO) is conducting tests with RU 486 and a similar drug (ZK98734, produced by Schering AG), but the status of the program is in question due to U.S. threats to stop funding all WHO programs if abortifacient and contraceptive research isn’t stopped.(5)
Without the California Food and Drug Bureau testing route, RU 486 probably wouldn’t be legally available in this country in the foreseeable future. The Bush administration has even gone so far as to prohibit the importation of RU 486 for personal use—something that has been allowed for other drugs. It is therefore unlikely that, without increased public pressure, the FDA would move quickly to accept RU 486 for testing if an application were ever received.
Tests funded by the Population Council have been conducted at the University of Southern California, but these tests might riot be acceptable under FDA licensing guidelines because of testing inconsistencies. Major U.S. drug companies have not shown interest in manufacturing the drug because of the high licensing and liability casts, and also because anti-choice groups have threatened to call for boycotts.
Small companies, non-profit organizations, or private individuals—all of whom wouldn’t be affected by boycotts and would have no assets for liability cases(6)—are the most likely candidates, other than the state of California, to undertake the licensing procedure for RU 486 and the necessary prostaglandin analogues. (PG analogues must be tested for use with RU 486 because the ones used in European tests are not licensed in the United States.)
Several small pharmaceutical companies across the country have demonstrated their interest in beginning the licensing process for both parts of the procedure, although Roussel-Uclaf has yet to respond to any of their offers.(7) Even if a group obtained the license and the FDA accepted the application, the testing procedure would probably take between five and ten years.
There are also several potential applications for synthesized anti-progesterone. Although development of these applications is still in the initial stages, some possibilities include: treatment for Cushing’s syndrome, glaucoma, meningiomas, breast cancer, and skin abrasions and bums. If a compound were licensed for any of these uses, it could be legally prescribed as an abortifacient.
Dangers for Women
A black market for RU 486 and analogous anti-progesterone compounds has already developed in the United States. This is dangerous not only due to the lack of quality control in manufacturing, but also because the drug has been proven safe and effective only up to the eighth week of pregnancy—with potentially disastrous results if used differently.
Furthermore, the 96 percent effectiveness of RU 486 is valid only for the procedure that includes a prostaglandin analogue. Without the prostaglandin, there is a success rate of only 50-85 percent, depending on what tests are used.
Overall advantages are few and far between The RU486 procedure is said to be safer than a surgical abortion and potentially less expensive. It can be administered by a private physician, it is widely viewed as less traumatic than a surgical abortion, and it allows a woman to abort in the privacy of her home. Some of these purported advantages do not actually benefit the majority of women, and others are simply untrue.
The claim that RU 486 is safer than surgical abortions is the first red flag. Many claims are made about new drugs concerning their safety, and these claims should always be examined cautiously.
Drugs such as DES* and the birth control pill were initially declared safe and devoid of significant side effects. It was obvious when they were introduced, and became more obvious in time, that they were fraught with problems—which affected the women who used them and their children. We still don’t know the full effects they will have on future generations. No one knows enough yet about RU 486 to make a definitive claim of safety.
Another potential danger in proclaiming an RU 486 abortion to be safer than a surgical one is the shadow such a notion casts over surgical abortion. It is an established fact that a first-trimester abortion performed legally and in medically safe conditions is one of the safest surgical procedures. In fact, surgical abortion carries a lower risk of death and complications than does a tonsillectomy; it is less risky than pregnancy or labor.
Access to safe and legal abortion is a fundamental demand of the reproductive rights movement internationally. Surgical abortions, which are safe and legal in the United States today, are not accessible to women around the world. Casting doubt on the safety of surgical abortions with the assumption that a new drug (which is % percent effective only before the eighth week of pregnancy) is safer undermines the effort of all women to gain control of our fertility. To use this procedure a woman must make a quick, informed decision and act on it. But this is a privilege not had by all women in this country or abroad.
In developing nations and other places where safe abortions are inaccessible or illegal, the use of RU 486 probably wouldn’t even make a dent in the more than 200,000 deaths per year from botched abortions. It would be, at best, an alternative back-street abortion—one done with a drug, without back-up medical facilities and without the medical supervision that is absolutely essential to the safety and effectiveness of this drug.
Especially when distributed by the Rockefeller Foundation or WHO, this drug is not an “option” for women. Advocating this “miracle drug” for use in developing countries ignores the fact that what is lacking in flue countries is a whole range of programs, from funding for health care to more equitable social and economic development—not a new option for abortion.
Population Control Device?
Not only are groups who are working to get RU 486 into this country using population-control rhetoric in their campaign, but an allied front consisting of women’s groups, family planning organizations, and population-control groups has formed around the issue.
While this may come as no surprise, it is underscored by the fact that the drug’s developer, Dr. Baulieu, has cited his own concern over what he calls the “complications of overpopulation” as a reason for the development of RU 486.(8) Only the efforts of a few socialist activists kept the National Organization for Women’s resolution to undertake an RU 486. Action Campaign from including Outreach to population-control groups.
It is true that the RU 486 procedure is a potentially less expensive alternative. The cost in France right now is about $125 (but because of the national health service, the woman does not pay the full amount). The relatively low cost of the RU 486 abortion is the main motivating factor behind testing the drug for national use in Britain and Sweden, for example. Doctors and planners in Britain see it as a way to reduce the hospital logjams that are responsible for many late, costly abortions. With RU 486, they estimate that the savings could be around 11 billion pounds a year.(9)
In China, it is estimated that the use of an anti-progesterone compound “could save millions of work weeks a year,” because it is assumed that women would no longer deserve the two–week paid leave they now receive after having an abortion.(10)
These potential savings are not lost on state governments or insurance companies in the United States, and were acknowledged at the San Francisco Board of Supervisors hearing on RU 486 in April. Of course, here in the United States, where nearly one-third of the population has no medical insurance and is not covered by any state funding, the savings would go to the woman paying for the procedure herself.
The danger of this cost-effectiveness is already being felt in Great Britain, where reproductive-rights activists fear that women wanting abortions before the eighth week of pregnancy (when RU 486 is effective) will not have the option of a surgical abortion. They will be forced to use anti-progesterone to save the government money.(11)
In addition, women who have suffered health problems related to past medical “advances,” and those of us who have learned from these experiences, may not want a medicated abortion. Every woman should have the option to choose between all available, safe methods, and this demand should be included in all efforts to get RU 486 into the United States.
The advantage that the drug can be administered by a private physician is good news for women who have private physicians. For millions of us who don’t, we would still go to clinics for the multiple visits required by the procedure, and we would face the same anti-abortion harassment and restrictive legislation that we do now.
Less Intrusive?
The RU 486 procedure has been characterized as being less traumatic because it is less intrusive than surgical abortions. Multiple visits to an office or clinic which include screening, tests, and examinations (as well as the possibility of a surgical abortion if the procedure is unsuccessful) still make this procedure quite intrusive. There would be, it seems, three visits required for the procedure in the United States, bypassing the waiting period mandated by French law before an abortion.
Currently there is work being done to develop a PG analogue that wouldn’t need refrigeration (which could, theoretically, cut another visit out of the procedure), but this is a long way away. Multiple visits will also make this procedure inaccessible to women who cannot afford numerous visits to the clinic or doctor’s office.
A health-care professional is required to monitor RU 486 usage, and at this stage, this is indeed necessary. But the existing legal procedure for the administration of RU 486 reinforces the control the predominantly white, male medical profession has over women’s bodies, control that has existed since the professionalization of medicine over a century ago.
Furthermore, any introduction of chemicals into the body is intrusive. The effects of synthetic hormone drugs like RU 486, although they stay in the body for a short time, are systemic. This drug still has many unexplained and unknown effects. The history of other “miracle drugs” such as DES, thalidomide, and the birth-control pill, as well as promising “advances” such as the Dalkon Shield, is instructive.
The lack of knowledge about these products demonstrates society’s general lack of concern for women through the haphazard, one-sided development and application of drugs, and a continued insufficient understanding of reproductive biology. This situation, which is no accident, has had disastrous effects and persists today.
The continued lack of concern for women is illustrated by the fact that testing done thus far has omitted any consideration of the psychological effects of RU 486 usage. One such study has been attempted in Great Britain,(12) but the results have not been compiled as of this writing. The unexplained effects of the drug, including hemorrhaging for up to thirty-five days, could cause a great amount of anxiety, as could the expulsion of the embryo without sufficient emotional support.
I have proposed that any testing done in California include a volunteer, comprehensive examination of the psychological effects on women. In this way, through its pioneering effort to establish testing in California, the City of San Francisco could indeed lead the nation by initiating an expanded study that demonstrates some kind of concern for women.
The Struggle Must Continue
Anti-choice forces see RU 486 as “chemical warfare” on the unborn, thinking that the apparent ease of the procedure will encourage women to have more abortions than we already have.
The use of synthetic anti-progesterones does indeed put limits on anti-choice protest tactics. The coercive use of developing fetuses in propaganda materials would be rendered meaningless by the fact that an RU 486-aborted seven-week embryo is not easy to detect and is expelled in a heavy menstrual flow.
However, attractive as this possibility maybe to some, it shouldn’t be primary motivation behind getting RU 486 licensed in the United States.
Most proponents of RU 486 toe the line of the medical establishment, downplaying the side effects and ignoring the inconsistencies and unknowns of the drug procedure. They concentrate on the monetary savings the procedure could bring about, and concentrate, above all, on the misconception that the procedure is private. They seem to want to develop a new construct around abortion to hide it.
Abortion is a difficult and, above all, personal choice to be made by a woman along with whomever she wishes to in-dude in her decision-making process. It is a personal choice but not a shameful one, not one that needs to be hidden, even if it were possible to do so. We all know the destructiveness of silence.
I believe that we must be realistic, examine this drug from every angle, and fight the stigma placed on abortion by right-wing propaganda.
No potential option for a safe abortion should ever be denied women. It has been established that RU 486 is being kept out of the United States for political and not medical reasons. Without an informed, cautious investigation, the technology of modern medicine will continue on and against us, not for our benefit.
Notes
- Pales, Joseph, “The Pill of choice,” Science, vol. 245, 13Z3.
back to text - Silvestre, Dr. Louise, et al, “Voluntary Interruption of Pregnancy with Mifepristone (RU 486) and a Prostaglandin Analogue: A Large-Scale French Experience,” New England Journal of Medicine, 322: 645-648.
back to text - “RU 486 Widening Choice for Women,” unpublished report on a Birth Control Trust conference at the Royal College of Obstetrics and Gynecology, London, 26 October 1989. Contraindications given by Dr. Louise Silvestre at this conference include anemia, any blood dotting disorders, chronic adrenal failure, long-term use of cortico-steroid therapy, anticoagulant therapy, and presence of renal or hepatic failure Asthma and severe hypertension are listed as additional contraindications to the prostaglandin in the NEJM report.
back to text - Statement made by California Attorney General John Van de Kamp, San Francisco Board of Supervisors hearing April 19, 1990.
back to text - Palca, 1321.
back to text - RU 486 is omitted from recent legislation introduced in Congress by Rep. Pat Schroeder (D-CO) to limit the liability companies must bear for their products.
back to text - One such company, Cabot Medical, was mentioned by Eleanor Bader in The Guardian (4/10/9O) as having agreed to produce the drug in the U.S. supposedly allowing NOW to effectively counter anti-abortion efforts to squelch distribution and production.” Mr. Warren Wood, president of the company, told me that he wishes this were the case. He has repeatedly contacted Roussel and been in effect told “don’t call us, we’ll call you.”
back to text - Women Wise staff, “RU 486: Major Topic at Conference, Women Wise, Winter 1986-87. The population-control viewpoints of Dr. Baulieu were given at a conference sponsored by Catholics for Free Choice in December 1986.
back to text - Veitch, Andrew, “Abortion Pill Put on Trial in 12 British Hospitals,” Guardian (GB), October 2 1987.
back to text - MacFarquhar, Emily, “The Case of the Reluctant Drug Maker,” U.S. News and World Report, Jan. 23, 1989, 54.
back to text - Unpublished report RCOG conference.
back to text - Ibid.
back to text
*Diethyistillbeatrol, a drug administered during lase pregnancy in the 1950s, which often led vaginal cancer in the pregnant women’s daughters.
July-August 1990, ATC 27